Introduction
Recent advances in three-dimensional (3D) reconstruction technology have been remarkable and are being used in various applications in medicine including navigation surgery, virtual reality-based surgery, and the education of students and residents [1]. In plastic surgery, 3D reconstructed images are mainly used in facial bone surgery [2]. Still, there are not many cases where they are applied to wound management and soft tissue-related diseases.
Among the various tomographic imaging studies, magnetic resonance imaging (MRI) is known to have excellent contrast even between various types of soft tissue and can easily provide image raw data for any plane direction including coronal, sagittal, axial and oblique, making it more suitable for evaluating soft tissue lesions than computed tomography (CT) [3]. Thinner sectioned images are required to reconstruct 3D images with better spatial resolution. In MRI, however, decreasing slice thickness lowers the signal-to-noise ratio and results in a grainy appearance. A thicker slice may improve image quality but reduces spatial resolution [4]. Therefore, MRI is unsuitable for 3D reconstruction of soft tissue lesions. In contrast, CT provides high resolution and good image quality without those tradeoffs; it is mainly used for 3D image reconstruction [5]. However, soft tissues are distributed within a narrow range between –100 and 100 Hounsfield units (HUs) in CT imaging with a value that overlaps with body fluids [6]. Due to this property, ordinary image acquisition and processing software cannot accurately discriminate the overlapping soft tissues within a narrow HU range.
Utilizing 3D reconstructed images of the region of interest (ROI) can aid preoperative surgical planning for debridement or resection of deeply located or vital structure-abutting wounds or lesions, and may also improve surgical outcomes by reducing complications and preventing unnecessary tissue damage during surgery. However, clinical application of 3D reconstructed images of wounds and soft tissue lesions has been limited to date due to the aforementioned characteristics of CT, the lack of automation, and the low spatial resolution of MRI. To overcome these limitations, surgeons can directly mark the ROIs on soft tissue tomography images and reconstruct them into a 3D image.
This study explicitly utilizes 3D reconstruction to effectively approach existing wound management and excision methods and presents such cases as examples. It introduces a method to easily create 3D images of wound extents and soft tissue lesions using open-source software and evaluates its usefulness through four clinical application cases. Clinicians underwent a hands-on course on how to use the software and apply it to clinical cases and completed a usefulness survey through questionnaires.
Methods
Basic concept and strategy
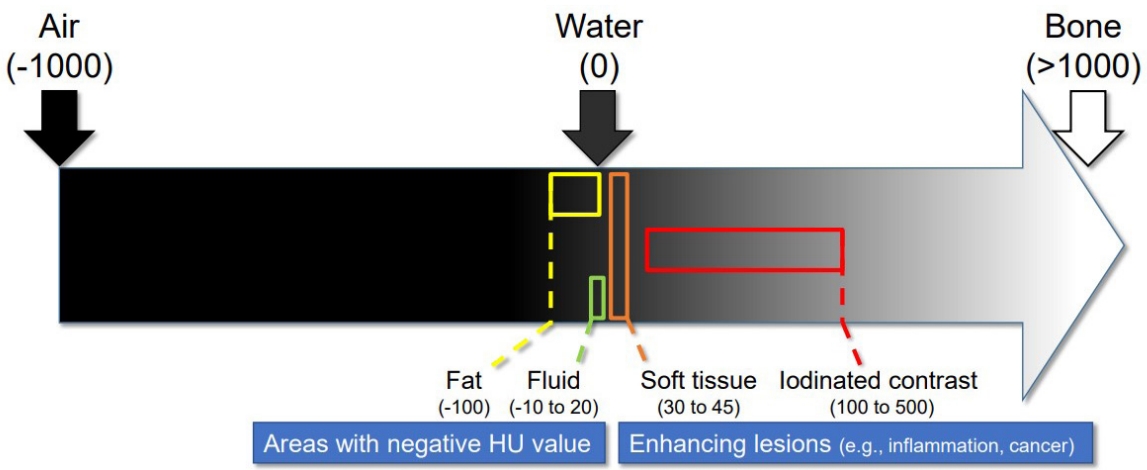
The HU, also called the CT unit, is calculated based on a linear transformation of the baseline linear attenuation coefficient of the X-ray beam [7]. Distilled water (at standard temperature and pressure) is arbitrarily defined as 0 HUs, and air is defined as –1,000 HUs [8]. Soft tissues and body fluids have a similar permeability to water. They are densely gathered within a narrow HU range, making it difficult to distinguish these lesions and reconstruct them in 3D images automatically. However, with contrast-enhanced CT images soft tissue lesions can be visually distinguished from the surrounding tissue, making it possible to reconstruct the lesion in 3D images. In this study, we hypothesized that using enhanced CT images would make it possible to manually distinguish and segment areas of interest such as fatty tissue and fluid cysts which have negative HU values, and inflammatory or recurrent cancer lesions which iodide contrast agents enhance with a higher HU value than the surrounding regions (Fig. 1). In this aspect, an open wound and the surrounding inflamed tissue can be a good candidate for segmentation as its HU values encompass both the negative HUs of fluid cysts (from wound discharge and purulence) and the enhanced higher HUs of inflammation. For MRI, we also hypothesized that manual markup on the ROI and reconstruction in 3D volume would aid in localizing lesions even with low spatial resolution.
3D image generation
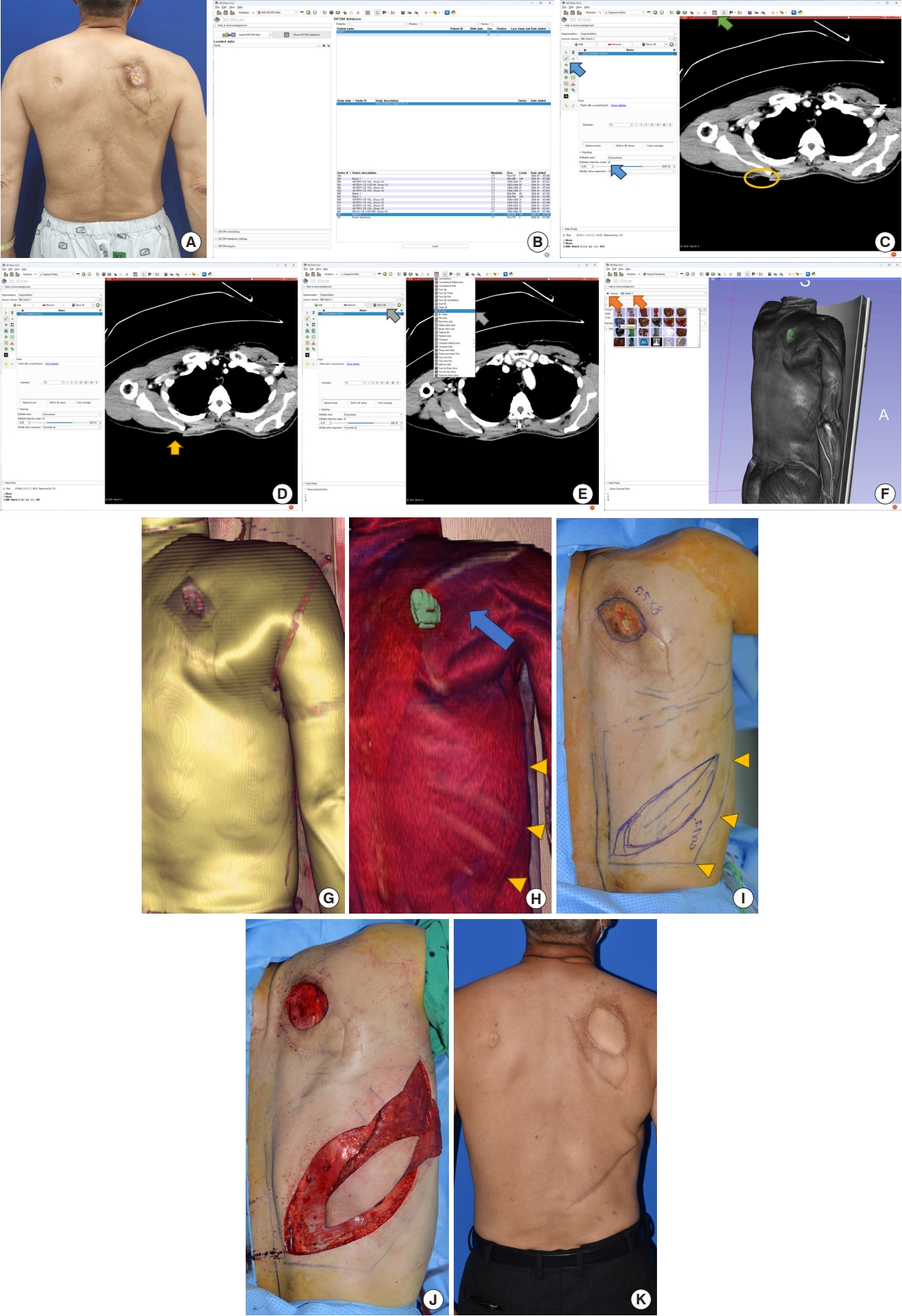
The Institutional Review Board of Incheon St. Mary’s Hospital reviewed and approved this study (IRB No. OC22QASI0078). Proper informed consent was obtained, and each patient was provided with an explanation of the procedure. The detailed steps for 3D image generation are hereby presented with a radiation ulcer patient as an example. The representative patient was a 62-year-old male who was referred to us after a failed keystone flap reconstruction of a 4×4 cm radiation ulcer on his upper back caused by prolonged percutaneous coronary intervention. Since the patient was on dual antiplatelet therapy, we postponed the definitive surgery for 6 months, during which conservative wound dressings contracted the ulcer to 2.5×3.5 cm (Fig. 2A). To prevent wound recurrence, precise estimation of the radiation damage and excision of the affected wound was a prerequisite for the final reconstruction. Because the extent of the radiation damage could not be determined with physical examination and the previously failed flap limited the arc of flap rotation, we decided to form a reliable debridement and reconstruction plan using a surgeon-generated 3D image.
The patients underwent a contrast-enhanced CT scan to evaluate the ROI. Depending on the target lesion, contrast-enhanced MRI could also be used. The tomography images were taken considering the future surgical position, putting the lesion superficially. After data anonymization, the surgeon downloaded the images from the picture archiving and communication system in a digital imaging and communications in medicine (DICOM) format. These images were further processed using 3D Slicer, a free, open-source software package for image analysis and scientific visualization (https://www.slicer.org/) [9].
The process of manipulation using 3D Slicer was as follows: the downloaded tomography image series were imported into 3D Slicer, and the enhanced cross-section images were selectively loaded (Fig. 2B). The “Segment Editor” module was chosen to distinguish the ROIs from the surrounding tissues (Fig. 2C). After adding new segmentation and naming, the cross-section view was prepared in the red slice window (Fig. 2C, green arrow). The surgeon could mark the ROI using a level tracer for delicate lesion tracing or a paint tool for faster marking. The enhanced radiation-injured ROI at the ulcer base was distinguishable (Fig. 2C, yellow oval). The surgeon marked this ROI using a paint tool with an editable intensity range (Fig. 2C, blue arrows). The marked ROI was shown in green (Fig. 2D, yellow arrow), and additional markings were made on the adjacent slices. After completion of markings, pressing the “Show 3D” button rendered the segmented area, and then it was visualized in the “3D only” mode viewer (Fig. 2E, gray arrows). At the “Volume Rendering” module, the surgeon could render the segmented area and the entire image simultaneously by selecting the source volume and activating it by clicking the closed eye icon (Fig. 2F, orange arrows). Selecting “Display-Preset” changed its render methods. By controlling the “Display-Shift,” the skin surface image with a rectangular dressing impression could be rendered (Fig. 2G). The deeper rendered image showed the segmented ROI (Fig. 2H, green) and its underlying musculature, denoting the anterior border of the latissimus dorsi muscle (Fig. 2H, yellow arrowheads). Note that the radiation-injured ROI was much larger than the cutaneous wound shown in Fig. 2G, indicating that a considerably larger extent of wound debridement would be required expected from the external appearance. The blue arrow designated the tunneling axis of the latissimus dorsi musculocutaneous flap, avoiding the previously failed flap (Fig. 2H).
The viewpoint of the reconstructed images was matched to the intraoperative field to design a narrow skin paddle and intraoperative debridement extent. The inferior angle of the scapula and latissimus dorsi muscle border (Fig. 2I, yellow arrowheads) were well-matched to Fig. 2H. The surgeon-generated 3D reconstructed image-assisted elevated flap and the defect are depicted in Fig. 2J. The postoperative clinical course was uneventful, as demonstrated in the postoperative 1-year photo showing the wound successfully covered by a stable flap (Fig. 2K).
In addition to the presented application, the final reconstructed 3D images can be overlaid on an anatomy plate [10] or clinical pictures after aligning viewpoint, coinciding scale, and increasing transparency. In this way, surgeons can reconstruct 3D tomography images with ROI markings and establish surgical plans more intuitively for approach to wounds and lesions of interest, thereby avoiding unnecessary injury to vital structures. In cases of infected wounds where debridement is often necessary, this method can be beneficial for preventing injuries to important structures and navigating effective drainage routes.
Evaluation of clinical applicability and efficacy of reconstructed 3D image in managing soft tissue pathologies
Our study focused on individual physicians who specialized in managing wounds or soft tissue lesions and might utilize 3D reconstruction for these conditions. The total number of specialists and residents registered in the Korean Society of Plastic and Reconstructive Surgeons in teaching hospitals was 624. The total number of medical doctors in Korea in the year 2021 was 109,937. Utilizing this information (P=0.0056) and applying Cochran’s sample size formula with a confidence level of 95% and a margin of error of 5% yielded an n-value of 8.556. Consequently, nine plastic surgeons were enrolled in hands-on training for the surgeon-generated 3D image reconstruction using tomography images and were surveyed. Participants were trained with lectures and hands-on courses with an instructor. Training evaluation was conducted using pre-training and post-training questionnaires to check any changes in the participants’ thinking before and after training (Table 1).
First, questions 1 to 9 were used to investigate changes in the perception of 3D reconstruction using tomography images. The Wilcoxon matched-pairs signed-rank test was performed on related questions. Questions 10 to 13 were added to the post-training survey to determine the usefulness and applicability of 3D reconstruction in clinical practice. The internal validity was calculated using the Likert scale for the survey results. Cronbach’s coefficient α values were calculated to assess the internal consistency and reliability of the content in questions 1 to 12. Then, a survey was included at the end of the questionnaire to find out which suggested example would be advantageous. The interval of validity was investigated using a linear numeric scale to see which case was the most useful among four cases for plastic surgeons in clinical practice. The Kruskal-Wallis test with Dunn’s multiple comparisons test was performed on related questions. Statistical analyses were performed with GraphPad Prism 9 (GraphPad Software).
Results
Clinical cases of surgeon-generated 3D reconstructed soft tissue lesions from tomography images
Case 1: I&D of a deep concealed pus pocket in a congenitally deformed foot severely scarred from multiple previous operations
A 35-year-old female patient visited the emergency room with erythema and swelling in her right foot, as well as a fever. She had a congenital club foot and had already undergone surgical reconstruction of an open foot wound twice due to recurrent infection. Initial CT evaluation revealed tenosynovitis with multiple abscess pockets in her foot. Incision and drainage (I&D) was performed based on physical examination and CT images, but the symptoms did not improve. Because of severe foot scarring from previous inflammation and surgery, it was difficult to check fluctuation and determine an appropriate incision site (Fig. 3). Finally, the abscess pockets were drained and cleansed using 3D reconstruction. The patient’s wound was covered with dermatotraction and a split-thickness skin graft.
Case 2: Removal of a deeply impacted foreign body in close proximity to a neurovascular bundle
A 42-year-old male patient visited the emergency room after a nail penetrated his hand. The nail had broken through, leaving a pinpoint opening just distal to the center of the distal wrist crease, and neurovascular injuries were expected based on the nail’s trajectory; moreover, the metallic foreign body hindered the use of MRI for visualization. Physical examination of the hand was unreliable due to severe pain and hyperventilation. The preoperative nail trajectory and its relative position to the neurovascular bundle had to be considered while determining surgical approach to avoid further damage and ensure safe removal of the foreign body (Fig. 4). These were identified preoperatively using 3D reconstruction. Finally, the surgeon could explore the cavity and remove the nail through a small 5 mm-extension incision of the original entry wound under loupe magnification, without any complications.
Case 3: Incision localization to prevent unnecessary tissue injury in biopsy of cancer-suspicious enhancing mass difficult to localize
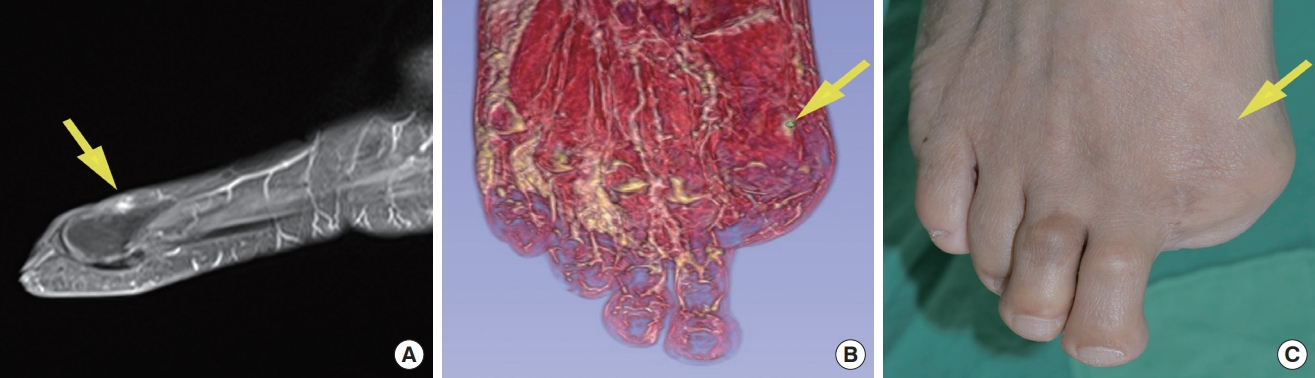
A 66-year-old male patient had his right big toe amputated because of a digital melanoma, after which follow-up imaging studies were used to check for recurrence. An enhancing lesion not present in the previous MRI was discovered, and since melanoma recurrence could not be ruled out based solely on the imaging, a biopsy was recommended. However, there was no palpable mass or externally distinguishable lesion, and it was impossible to locate the suspicious lesion clinically for surgical excision (Fig. 5). Surgical biopsy was performed aided by 3D reconstruction of the lesion location. With a lesion-focused precise incision, this prevented unnecessary excessive surgical injury. Pathology revealed a focal nodular inflammation. The enhancing lesion had disappeared on the follow-up MRI examination, and there was no recurrence of melanoma for 5 years after that.
Case 4: Effective approach planning for deep-seated cancer-suspicious mass abutting vital structures
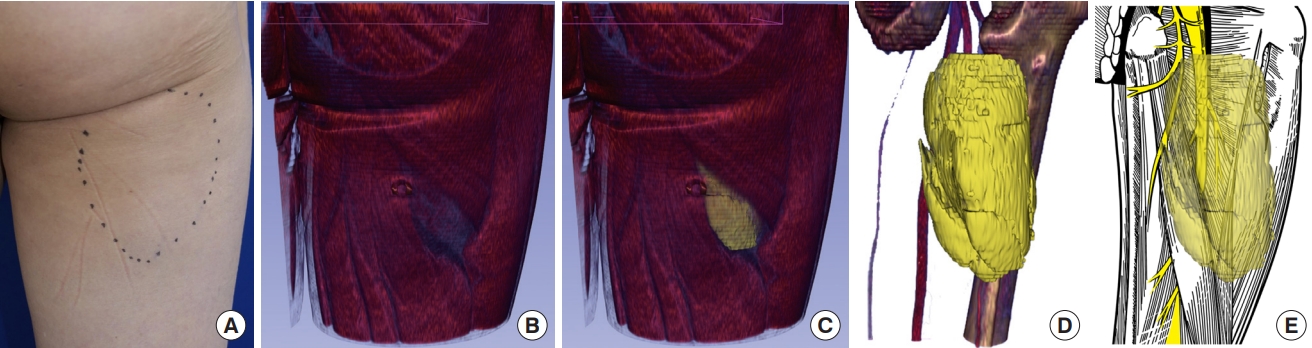
A 59-year-old male patient complained of long-lasting vague discomfort on his right posterior thigh which was found to be caused by a deep palpable mass. Initial evaluation with a contrast-enhanced CT image revealed a deeply seated huge mass in the posterior compartment of the thigh. The mass displaced the sciatic nerve and vascular bundles and was cleaved into two parts. Inhomogeneous attenuation within the huge mass suggested liposarcoma. 3D reconstruction was used to form an effective incisional plan for wide resection of the mass while avoiding muscle and neurovascular injury (Fig. 6). An approach between the lateral border of the long head of the biceps femoris and the inferior border of the gluteus maximus was chosed as this avoided vital structures and allowed even approach to the cleaved mass. After surgery, the patient healed without complications, and the mass was diagnosed as a liposarcoma with clear resection margins. There was no recurrence of the tumor after 5 years of follow-up.
Analysis of pre-training and post-training questionnaires
Participants were four plastic surgery residents and five board-certified plastic surgeons, of which one had clinical experience of less than 5 years, two between 5 and 10 years, and two with more than 10 years. For responses to questions 1 to 9, both the pre-training group (Cronbach’s α=0.91) and post-training group (Cronbach’s α=0.86) exhibited Cronbach’s α values higher than 0.7 [11], indicating satisfactory internal consistency. For questions 10 to 12, the α values (Cronbach’s α=0.75) confirmed the reliability of this survey.
Although there were tendencies of a general increase of the scores from question one to nine in the post-training group, they showed no significant change in participants’ perception of applying 3D reconstruction in soft tissue lesions after the hands-on training. However, answers to the question of whether the use of 3D reconstruction in deep soft tissue lesions would help the surgical outcome (question 6) showed a statistically significant result: the answer “likely” before the training changed to “very likely” after the training (P<0.05) (Fig. 7).
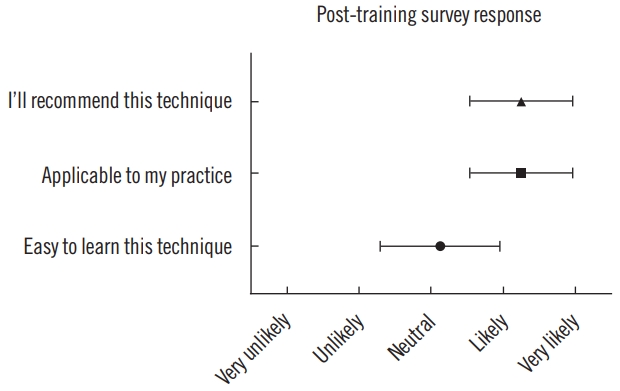
Fig. 8 shows the results for questions 10 to 12. There were positive answers regarding whether to recommend 3D reconstruction and apply it to clinical practice, but opinions were neutral on whether it is easy to learn.
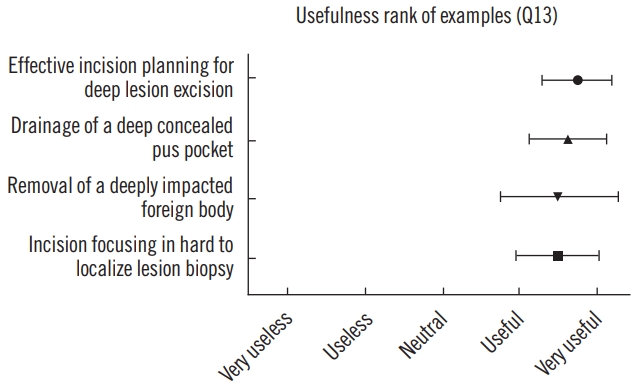
Question 13 evaluated which case 3D image reconstruction was judged to be the most useful among the four cases presented in training. The results showed that it would be the most clinically useful for deep lesion excision planning, followed by drainage of deep pus pockets, removal of foreign bodies, and hard-to-localize-lesion biopsy. However, there was no statistically significant difference (Fig. 9).
Discussion
3D reconstructions of patient images have been utilized in various clinical applications. In plastic surgery, 3D CT reconstruction has been mainly used for facial bone surgery because the HUs of bone are easily discriminable from the surrounding tissue [12].
In contrast, 3D CT reconstruction of wounds and soft tissue lesions is more challenging because the HUs of soft tissue have little difference from the HUs of the surrounding tissue [6]. Research on the 3D reconstruction of soft tissue lesions began in the 1990s, when MRI, which can easily image soft tissue, was commercialized. Chu et al. [13] published a study that aided the treatment of temporomandibular joints by using 3D reconstruction of MRI scans. However, the disadvantages of MRI are low image quality due to large voxels, high cost, and limited accessibility [4]. With the development of contrast medium technology, it was possible to make a sufficient contrast difference with the surrounding tissue in vital organs with abundant blood flow [14].
As mentioned above, the contrast difference in wounds and soft tissue lesion images is insufficient to find the ROI, making it difficult for image processing software to automatically reconstruct these in 3D. Therefore, instead of the previous approach which delegated the job of automatically finding the ROI to image processing software, we performed 3D reconstruction by having a physician manually mark the ROI in the wound or soft tissue lesion. The difficulty of the reconstruction process and its clinical utility were objectively investigated in the form of a questionnaire. This is the first study that clinically applied 3D reconstruction by having physicians directly mark the ROI on soft tissue lesions that can be distinguished on tomography images.
According to the survey results, plastic surgeons positively evaluated 3D reconstruction technology even before training. However, only in the question of whether the 3D images of deep soft tissue lesions would help improve surgical outcomes (fewer incisions, less bleeding, complete removal, etc.) did the answer change statistically significantly from likely to very likely. This result implies that plastic surgeons had difficulty determining incision plans and experienced unsatisfactory surgical outcomes when operating on deep soft tissue lesions.
There were positive answers about recommending 3D CT reconstruction or applying it to clinical practice, but there were many neutral answers regarding the ease of learning. These results originated from the inconvenience that more than one program must be used to extract the DICOM files and render the 3D reconstruction, and a surgeon must manually select the lesion to be reconstructed from the CT image. It also showed that it might be difficult for clinicians to learn how to use the open-source software. However, we should keep in mind that each person has different computer skills and clinical experiences.
As in the first case, which entailed I&D on a patient with clubfoot, finding the appropriate external approach site to a deep lesion may be challenging if the patient has a large amount of scar tissue or tissue adhesion as a result of several past surgical procedures. 3D CT reconstruction may provide more information for preoperative planning compared to the limited utility of physical examination on deformed and scarred anatomical structures. This may be even more beneficial in cases when a free flap is considered after debridement, since preserving the major blood vessels around the lesion is of utmost importance.
This technology may also be helpful, as in the second case, when exploration is needed for foreign body removal. As in the third case, for contrast-enhancing lesions suspicious of cancer recurrence but without any external signs such as skin wounds or pigmentation and indistinguishable on ultrasonography, 3D images can help surgeons determine the optimal incision location for biopsy, avoiding unnecessary dissection and tissue damage, even with low spatial resolution MRI. Finally, when excising deep soft tissue lesions, there are many things to consider preoperatively, such as the direction of the incision and the surrounding major vital structures such as blood vessels and nerves. 3D CT reconstruction helps the surgeon orient these deep and complex structures and plan an effective approach simultaneously.
As shown in the above cases, it is difficult to specify the exact surgical site with tomography images alone. Surgery can be performed more efficiently by matching 3D reconstructed images the operator’s field of view, specifying the exact ROI. Moreover, surgeons can easily implement this method using open-source software through training without the help of experts or additional costs for professional software.
The time required for segmentation varies depending on the operator’s proficiency in 3D Slicer, the level of precision required for each clinical case, and the size of the target object. For skilled practitioners, the working time was within 5 minutes per case, after which they could use the reconstructed image to effectively establish a surgical plan before surgery. Study participants were initially able to complete the task within approximately 20 minutes, and they could shorten the duration through repeated practice. In this study, segmentation was performed based on visually identifiable areas, utilizing a painting rather than level tracing. Although precision decreased, the segmentation could be completed quickly. When aiming for higher precision by opting for level tracing, it requires performing segmentation more meticulously by finding similar HUs using the level tracing function of the imaging software. This method is used in cases where more precise segmentation is needed, such as cancer cases like case 3.
Surgical navigation and artificial intelligence (AI) are also actively being studied and implemented as novel approaches to reconstructing surgical sites [15]. However, intraoperative navigation systems are usually used for tracking bone or ligament structures [16]. Unlike these rigid anatomical structrures, soft tissue lesions are subject to significant shifts and deformation due to factors such as breathing, heartbeats, patient movement, and surgical manipulation, resulting in inaccurate coordinate registration between the image and the patient. For these reasons, soft tissue intraoperative navigation systems still have limitations [17].
The integration of AI into 3D reconstruction of medical images is considered an innovative breakthrough [18]. Deep learning (DL)-based methods explore representative features from medical images in an adaptive manner, unlike traditional methods that rely on handcrafted features [19]. DL-based image segmentation is mainly used for the segmentation of large or multiple organs. In general, this technique is more effective for organs that have a large size and a regular distinctive shape, such as the lungs and heart, and less useful for small objects. In addition, clinical data processing and network training are required, and post-processing of the results of DL segmentation is necessary in most cases [20]. Therefore, DL-based wound or soft tissue lesion segmentation is limited due to the insufficient number of training sets that can accommodate the various anatomical locations and physical characteristics of each specific lesion targeted by the surgeons’ diverse needs. While AI is currently applicable to CT reconstruction for structures with well-defined HU threshold values such as bones or calcified masses, its effectiveness in replacing direct intervention is challenging in cases involving diverse HU differences or signal intensity values in soft tissue [21]. Although Yang et al. in 2023 [22] could reconstruct soft tissue by utilizing AI for the segmentation of 3D gingival images in an animal study, this was achieved by excluding the AI-segmented bone and teeth structures from the reconstructed composite of the teeth and gingiva, and not by actual AI-segmentation of gingival soft tissue. Considering these limitations of surgical navigation and AI technology, we believe that our suggested methods can assist clinicians in wound management and surgical planning until navigation and AI technology are further developed to enable more precise navigation and segmentation.
This method has some limitations. First, due to soft tissue deformability, errors may occur in which the actual lesion’s location does not precisely match the tomography image’s location spatially. In addition, it is difficult to use this method when the quality of the tomography is low. The last limitation is the small number of participants who answered the questionnaires to evaluate the efficacy of this study.
In conclusion, 3D image reconstruction using open-source software can be easily accessed by clinicians and applied to clinical practice. 3D images can be used in various ways for wound management, resection, and drainage surgery, even in soft tissue lesions where 3D images have not been applied readily in the past. Despite the limitations of this method, it could aid surgeons to preoperatively plan and improve surgical outcomes in managing deep soft tissue lesions.